
Managing Knee Osteoarthritis Through Evidence-Based Loading Programs: Overcoming the Fear of Movement

For thousands of individuals across Ontario, a diagnosis of knee osteoarthritis (OA) feels like a physical dead end. It is incredibly common for patients to be told that their joints are simply “wearing out,” leading to the frightening belief that their knee is a mechanical hinge with a finite number of bends left. This “bone-on-bone” narrative naturally triggers intense kinesiophobia—a deeply ingrained fear of movement. To protect the aching joint, patients stop walking, avoid stairs, and abandon active lifestyles.
However, modern sports medicine and orthopedic research show that complete rest is actually one of the worst choices for an arthritic joint. Your knee cartilage is not a static piece of plastic that wears away with use; it is a dynamic, living tissue that thrives on physical stress.
By overcoming the fear of movement and engaging in an evidence-based progressive resistance loading program, patients can actively stimulate their body’s natural joint lubrication system. This clinical breakdown explains the underlying fluid biology of the knee and outlines how structured exercise helps manage osteoarthritis pain.
1. The Living Matrix: How Cartilage Breathes Through Compression
To understand why loading your knee is therapeutic, we must first look at how articular cartilage receives its nourishment. Unlike your muscles, skin, and bones, the hyaline cartilage capping the ends of your femur and tibia has no direct blood supply. It cannot pull oxygen and nutrients directly from the bloodstream to heal or maintain itself.
Instead, cartilage relies entirely on a mechanical fluid exchange process known as interstitial fluid flow, which functions exactly like a commercial kitchen sponge:
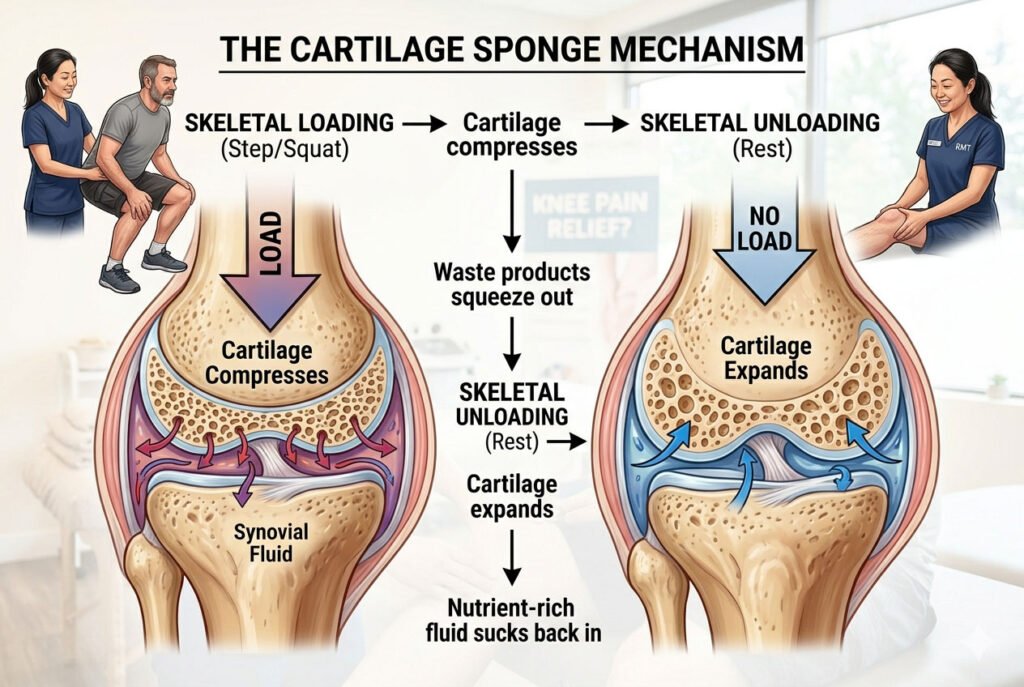
When you put weight on your knee during a controlled exercise, the cartilage matrix compresses. This pressure pushes cellular waste products out of the tissue and into the surrounding synovial fluid chamber. When you remove that weight, the cartilage expands back to its resting size, acting like a vacuum to pull fresh, nutrient-dense fluid back deep into its cellular matrix.
If an individual avoids moving due to pain, this vital fluid exchange grinds to a halt. The cartilage becomes chronically starved of nutrients, accelerating cellular breakdown and making the joint increasingly stiff, brittle, and sensitive to everyday movements.
2. Stimulating the Joint’s Lubrication: Aggrecan and Lubricin Dynamics
Progressive strength training does more than just feed the cartilage; it actively triggers the production of high-performance biological lubricants inside the joint capsule.
When a joint capsule experiences the rhythmic, mechanical compression of structured resistance training, the specialized cells within the synovial membrane respond by increasing the synthesis of two vital lubricating molecules:
Hyaluronan and Lubricin
Lubricin is a dedicated boundary-lubricating protein that forms a slippery protective coat over the surface of your cartilage. Working together with hyaluronan, it ensures your bones glide past one another with a coefficient of friction that is slicker than ice sliding on ice. Controlled physical loading actively signals the joint lining to secrete a fresh, thick wave of this fluid mixture.
Aggrecan and Proteoglycan Density
Deep within the cartilage matrix live large molecules called proteoglycans, with the most vital being aggrecan. These molecules act like microscopic water magnets, trapping water molecules tightly inside the tissue to give the cartilage its bouncy, shock-absorbing qualities. Clinical loading programs stimulate the cartilage cells to build more of these water-binding molecules, directly increasing the compressive strength and resilience of the joint.
3. The Phased Timeline for Safe Knee Loading
Overcoming osteoarthritis pain requires a careful, structured progression that gradually builds up your tissue tolerance without overloading the joint.
1.Phase 1: Pain Desensitization and Isometric Base: Weeks 1 to 4.
Clinical Focus: Lowering nervous system threat perception and activating the quad muscles without aggravating joint surfaces.
Exercises utilize isometrics—holding a muscle contraction without moving the joint, such as a wall sit or a straight-leg raise with a brief hold. This provides an immediate pain-relieving effect within the nervous system while building initial muscle endurance.
2. Phase 2: Closed-Kinetic-Chain Hypertrophy: Weeks 5 to 12.
Clinical Focus: Rebuilding the quadriceps, hamstrings, and gluteal muscle mass to absorb impact forces.
Patients progress to slow, controlled movements where the foot stays planted on the ground, such as shallow leg presses, box squats, and Romanian deadlifts. These exercises are performed through a comfortable, pain-free range of motion to stimulate fluid exchange and thicken the surrounding muscle fibers.
3. Phase 3: Rate of Force Development and Power: Month 3+.
Clinical Focus: Training the lower limb muscles to react quickly and absorb sudden impacts during daily life.
Training introduces faster, dynamic movements like stepping up onto elevated platforms, controlled lateral walking with resistance bands, and progressive split squats. This phase ensures the knee can easily handle sudden changes in footing on uneven pavement or stairs.
Clinical Reality: The Traffic Light Pain Monitoring System
A major barrier to recovery is the belief that a successful workout must be completely pain-free. When patients experience a minor ache during an exercise, they often assume they are causing structural damage and stop immediately.
To help patients manage this safely, clinicians utilize a simple, objective Traffic Light Protocol to track acceptable discomfort during active loading:
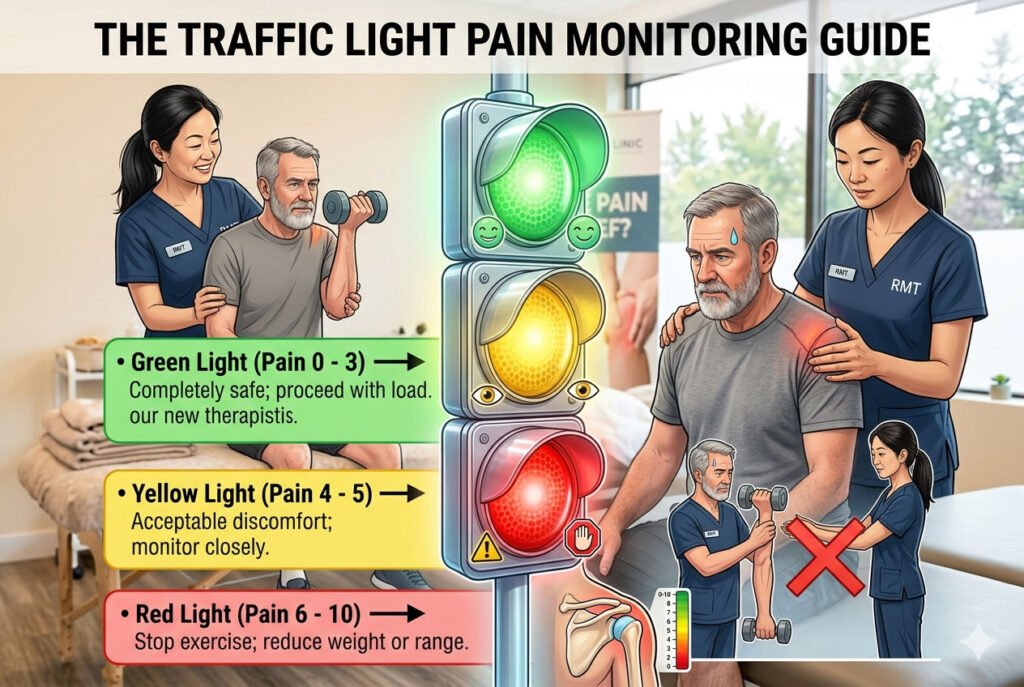
Discomfort within the Yellow Zone (4 to 5 out of 10) is a normal, safe part of remodeling a chronic joint condition. The absolute rule for safety is that any discomfort experienced during the workout must return to its baseline level within 24 hours. If your knee feels significantly more achy or swollen the following morning, it simply means the mechanical load was slightly too high, and the next session should be adjusted with lighter weights or a smaller range of motion.
The Power of a Connected, Coordinated Approach
Reversing the cycle of knee osteoarthritis requires addressing both the structural joint changes and the surrounding soft tissue networks. When a knee joint is chronically stiff, the surrounding muscles—especially the calves, quadriceps, and IT band—often tighten up defensively to guard the leg. This constant muscle tension creates a compressing force across the joint capsule, which can worsen daily pain.
Within our care network, we manage osteoarthritis through a collaborative, multi-disciplinary model. While a Physical Therapist or Chiropractor maps out your specific movement tolerances and designs your progressive loading program, a Registered Massage Therapist (RMT) can simultaneously use deep myofascial release, trigger point therapy, and Swedish massage to loosen hyperactive, guarded muscles and flush away localized swelling.
Every stage of your strength testing, range of motion improvements, and daily pain trends is documented in secure digital health charts (SOAP notes), keeping your entire care team perfectly unified. By combining targeted soft-tissue therapies, expert biomechanical loading, and practical pain education, our team addresses both your muscular comfort and joint health at the same time—giving you a clear, confident path to move freely, protect your cartilage, and reclaim your active life.

Author: Henry Tse
Henry Tse, Founder and CEO of the RMT Clinic Network Organization—an integrated platform created to connect patients with trusted para-medical providers while helping practitioners build stronger, more profitable clinics using practical, real-world business systems. After launching, operating, and selling multiple wellness businesses, I repeatedly saw the same two challenges: patients struggled to find the right care close to them, while practitioners struggled to attract consistent bookings and build predictable, compliant, and sustainable businesses. I created the RMT Clinic ecosystem to solve both problems. Through our Canada-wide “near me” directory, specialized brand marketing solutions, and step-by-step training academy, we help patients discover qualified providers while giving Registered Massage Therapists and clinic owners the systems, tools, and strategies needed to turn their professional skills into scalable businesses. Core Values Innovation • Empowerment • Community Professional Background * Vice President and General Manager, Canadian Small Business Institute: 15 years as a senior business consultant and trainer. * Direct Marketing and Advertising, 1997–Present: Strategy, brand positioning, lead generation, and business development. * Wellness Clinic Owner and Operator, 2005–Present: Launched and operated nine clinics, with three active RMT clinics currently under management. If you are an RMT or clinic owner looking for more bookings, stronger...