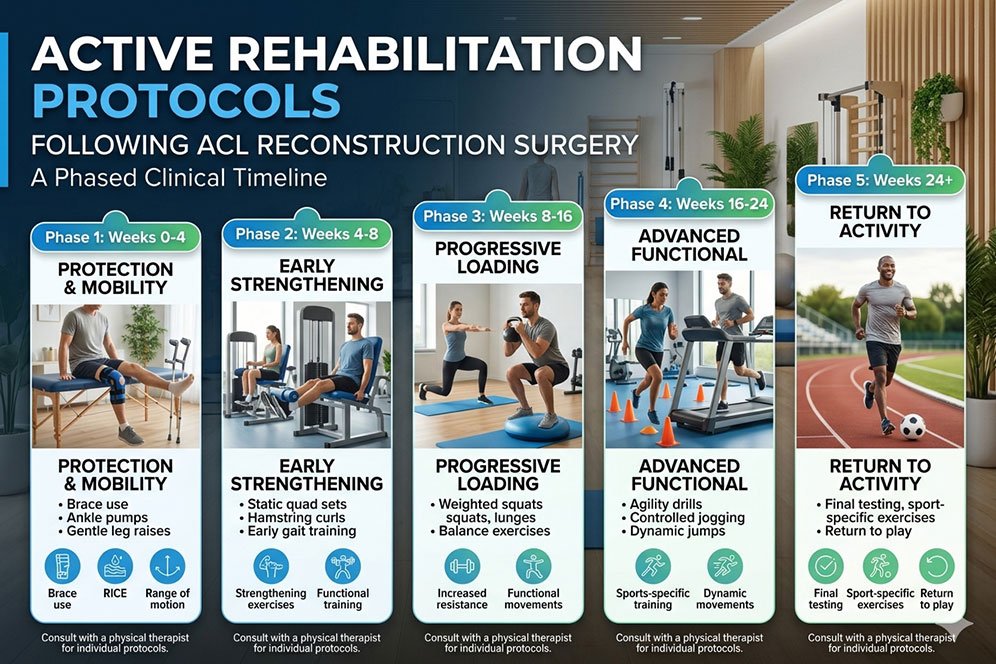
Active Rehabilitation Protocols Following ACL Reconstruction Surgery: A Phased Clinical Timeline
An Anterior Cruciate Ligament (ACL) rupture is one of the most significant orthopedic disruptions an athlete or active individual can face. Whether the injury occurred on a volleyball court in Willowdale or during a soccer match in the Greater Toronto Area, the path forward requires a meticulous, evidence-based approach. Surgery is only the first step; the true key to a successful return to sport or daily activity lies in a structured, multi-phase active rehabilitation protocol.
In Canada’s regulated healthcare landscape, rehabilitation is no longer guided by guesswork or pain levels alone. Modern sports medicine relies on strict, objective milestones that respect the biological healing timeline of the newly grafted ligament.
By coordinating targeted physical therapy, progressive strength training, and specialized clinical manual therapy, patients can safely navigate the long journey from early weight-bearing to final agility testing. This comprehensive guide outlines the vital clinical phases required to optimize knee stability and ensure a safe return to peak performance.
1. The Biology of the Graft: Respecting Ligamentization
To understand why a phased timeline is critical, it is essential to look at the biology of the ACL graft. During surgery, the ruptured native ligament is replaced with a tissue graft—most commonly harvested from the patient’s own patellar tendon, hamstring tendon, or a donor tissue (allograft).
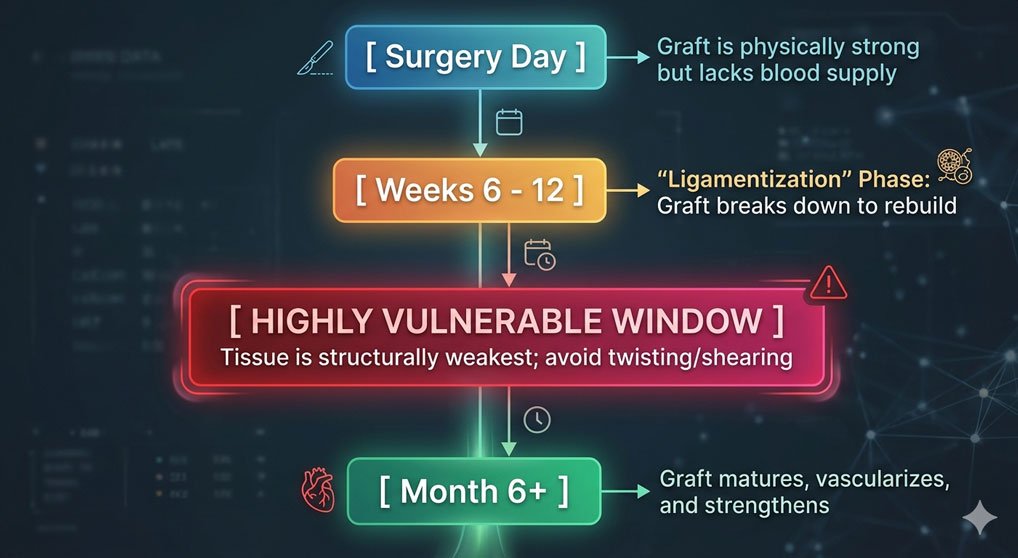
Initially, the graft is mechanically strong because it is securely anchored into the femur and tibia bones with surgical screws. However, between weeks 6 and 12, the graft undergoes a profound biological shift called ligamentization. During this phase, the original cells die off so that your body can flood the area with new blood vessels and lay down fresh collagen.
During this middle window, the graft is actually at its structurally weakest point, even though the patient’s knee may feel completely pain-free and stable. Introducing aggressive twisting movements or heavy open-kinetic-chain knee extensions too early can permanently stretch out or rupture the healing graft.
2. Milestone-Driven Active Rehabilitation Timeline
A successful clinical care plan must progress based on objective structural milestones rather than a generic calendar schedule.
The Structural Foundation
Phase 1 (Weeks 1 to 4): Protection & Early Motion
Clinical Focus: Protecting the healing graft, eliminating swelling, and achieving full knee extension.
Safety Protocols: The immediate goal is restoring a normal walking pattern. Patients focus on early weight-bearing as tolerated while using a protective brace. Regaining full passive knee extension (getting the leg completely straight) is vital; failing to achieve a straight leg in the first month can lead to permanent scar tissue buildup and a lifetime of limping.
Building the Muscular Support
Phase 2 (Weeks 5 to 12): Progressive Strengthening
Clinical Focus: Rebuilding quad mass, restoring a full range of motion, and normalizing balance.
Safety Protocols: As joint swelling drops, exercise shifts to closed-kinetic-chain movements where the foot stays planted on the ground, such as leg presses and shallow squats. Therapists pay close attention to the hamstrings and quadriceps, ensuring they fire together symmetrically to protect the knee joint.
Introducing Impact Load
Phase 3 (Weeks 12 to 20): Running & Plyometrics
Clinical Focus: Transitioning to straight-line running and introducing low-impact jumping mechanics.
Safety Protocols: Before a patient is allowed to jog, they must demonstrate that their surgical leg has regained at least 70% of the strength of their uninjured leg during testing. Training focuses heavily on eccentric control—teaching the muscles how to absorb landing shock safely without letting the knee buckle inward (valgus collapse).
The Final Clearance
Phase 4 (Month 5+): Agility & Return-to-Sport
Clinical Focus: Multi-directional cutting, high-velocity deceleration, and sport-specific drills.
Safety Protocols: This phase prepares the athlete for the chaotic, unpredictable movements of competitive sports. Patients undergo a rigorous Return-to-Sport Testing Battery to confirm the knee is fully ready for intense activity.
3. Advanced Criteria-Based Testing for Final Sports Clearance
Clearing a patient to return to competitive sports like volleyball, soccer, or basketball is the highest-risk decision in sports medicine. Historically, doctors cleared patients based on a simple calendar mark, like “six months post-op.” This outdated approach resulted in high re-injury rates.
Today, clinicians within our network utilize a strict, objective Return-to-Sport Testing Battery that patients must pass before getting cleared to play:
1. Isokinetic Strength Testing
The quadriceps and hamstring muscles act as the primary protectors of the ACL graft. Using specialized equipment, we measure total muscle torque. The surgical leg must achieve a Limb Symmetry Index (LSI) of 90% or higher, meaning it is nearly identical in power to the uninjured leg.
2. Functional Hop Testing Sequence
Patients perform a series of intense, single-leg hop tests over a measured distance:
- Single Hop for Distance: Measuring raw explosive power.
- Triple Hop for Distance: Evaluating consecutive landing control.
- 6-Meter Timed Side-Hop: Testing rapid lateral stability and endurance.
The distance jumped and the quality of the landing mechanics must score above a 90% symmetry match. If the knee wobbles or collapses inward during a landing, clearance is held back until stability improves.
Clinical Reference: ACL Rehabilitation Progress Matrix
To help patients and clinic managers monitor recovery milestones, this clinical reference table outlines how treatment parameters adapt across the healing journey:
| Recovery Phase | Primary Movement Goals | Open vs. Closed Chain Rules | Manual Therapy Support Focus |
|---|---|---|---|
| Phase 1 (Wk 1-4) | Achieve full straight leg; activate quads | Closed-chain weight-bearing as tolerated | Manual patellar gliding; gentle lymphatic drainage |
| Phase 2 (Wk 5-12) | Restore full knee bend; build base strength | Strict closed-chain focus; avoid heavy open-chain leg extensions | Myofascial release of hamstrings and calves |
| Phase 3 (Wk 12-20) | Straight-line jogging; basic jumping patterns | Progressive entry into light open-chain movements | Scar tissue mobilization around surgical incisions |
| Phase 4 (Month 5+) | Sharp cutting and pivoting; explosive sport drills | Full open and closed-chain integration under high loads | Neuromuscular coordination retraining |
The Value of Coordinated Multi-Disciplinary Rehabilitation
Recovering from an ACL reconstruction is a long process that requires targeting both the joint structures and the surrounding soft tissue networks. Muscles cannot gain strength efficiently if they are bound up by painful knots, and joints cannot move smoothly if they are restricted by thick post-surgical scar tissue.
Within the RMT Clinic Network, we navigate complex sports recoveries using an integrated, collaborative care model. While a Physical Therapist or Chiropractor guides your active exercise progression, a Registered Massage Therapist (RMT) can simultaneously utilize advanced myofascial release, scar tissue mobilization, and targeted trigger point therapy to release the intense muscle tension that develops from shifting your weight during recovery.
Every single assessment, strength score, and movement milestone is carefully logged in secure digital health charts (SOAP notes), keeping your entire sports medicine team perfectly aligned. This unified approach balances joint mechanics, muscle mass, and soft-tissue health simultaneously—giving you a safe, reliable path to clear your testing, protect your graft, and confidently step back onto the field.

Author: Henry Tse
Henry Tse, Founder and CEO of the RMT Clinic Network Organization—an integrated platform created to connect patients with trusted para-medical providers while helping practitioners build stronger, more profitable clinics using practical, real-world business systems. After launching, operating, and selling multiple wellness businesses, I repeatedly saw the same two challenges: patients struggled to find the right care close to them, while practitioners struggled to attract consistent bookings and build predictable, compliant, and sustainable businesses. I created the RMT Clinic ecosystem to solve both problems. Through our Canada-wide “near me” directory, specialized brand marketing solutions, and step-by-step training academy, we help patients discover qualified providers while giving Registered Massage Therapists and clinic owners the systems, tools, and strategies needed to turn their professional skills into scalable businesses. Core Values Innovation • Empowerment • Community Professional Background * Vice President and General Manager, Canadian Small Business Institute: 15 years as a senior business consultant and trainer. * Direct Marketing and Advertising, 1997–Present: Strategy, brand positioning, lead generation, and business development. * Wellness Clinic Owner and Operator, 2005–Present: Launched and operated nine clinics, with three active RMT clinics currently under management. > If you are an RMT or clinic owner looking for more bookings,...