Pelvic Floor Physiotherapy for Post-Partum Core Stabilization

A Trauma-Informed Introduction
Bringing a child into the world is a profound, life-altering experience. Yet, for many post-partum individuals across the Greater Toronto Area, the months following childbirth can bring unexpected physical vulnerabilities. Symptoms like urinary leakage when laughing or lifting, a persistent “doming” down the center of the abdomen (diastasis recti), deep pelvic pressure, or pain during intimacy are incredibly common—yet they are rarely discussed openly.
Far too often, new parents are told that these issues are simply a “normal part of having a baby” and are advised to just do generic Kegel exercises. However, clinical sports medicine and pelvic health research show that post-partum issues are rarely fixed by basic contractions. In fact, blindly tightening the pelvic floor can sometimes make the problem worse.
True post-partum recovery requires a gentle, trauma-informed approach that addresses the entire core system. By treating pelvic floor health through specialized clinical assessment, manual therapy, and structural muscle re-education, individuals can safely rebuild their core stability from the inside out.
1. The Core Cylinder: Managing Your Internal Pressure System
To understand post-partum recovery, we must stop viewing the abdominal muscles and the pelvic floor as isolated parts. Clinically, your torso functions as an integrated deep core cylinder, or a closed pressure system.
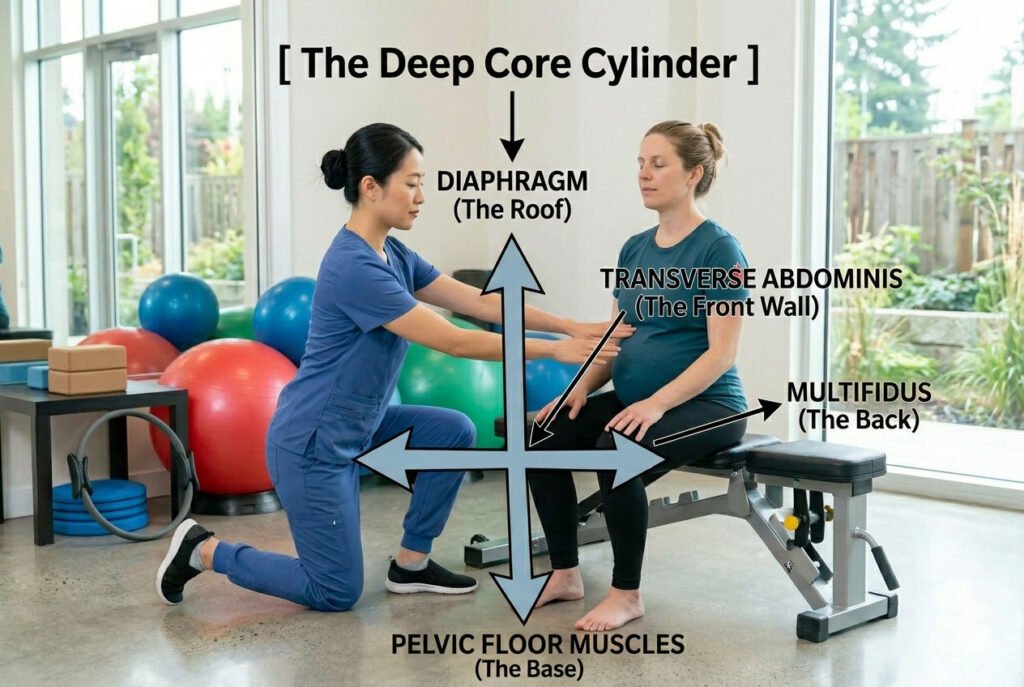
This pressure system relies on four structural walls working in perfect harmony:
- The Roof: The respiratory diaphragm (your breathing muscle).
- The Base: The pelvic floor muscles (the sling supporting your bladder, uterus, and bowel).
- The Front Wall: The transverse abdominis (your deepest, corset-like core muscle).
- The Back Wall: The multifidus (the deep stabilizers along your spine).
During pregnancy, the massive physical expansion of the uterus stretches the front wall to its absolute limit, altering the mechanical pull on your spine and pelvis. When you breathe in, your diaphragm drops down, naturally increasing the pressure inside your abdomen. In a balanced system, the pelvic floor gently stretches downward to absorb this pressure, then rebounds naturally as you breathe out.
If the front wall remains overstretched or weak after birth, this natural pressure management breaks down. Instead of distributing the load evenly, internal pressure slams downward directly into the pelvic floor or pushes outward against the healing abdominal midline. This uneven pressure is what causes core instability, low back aches, and pelvic organ prolapse.
2. Understanding Pelvic Floor Hypertonicity: The High-Tone Myth
There is a widespread misconception that post-partum leakage or weakness always means the pelvic floor muscles are stretched out, floppy, and “too loose.” This assumption leads many individuals to perform hundreds of rapid Kegel contractions daily.
However, clinical evaluations frequently reveal the exact opposite issue: Pelvic Floor Hypertonicity (an overactive, high-tone pelvic floor).
When the larger, global core muscles become weak or uncoordinated during pregnancy, the deep pelvic floor muscles often tighten up defensively to hold the pelvis stable. This means the tissue is chronically shortened, locked, and exhausted.
A muscle that is already locked in a tight contraction cannot contract further to absorb a sudden spike in pressure—such as a cough, a sneeze, or a heavy lift. This functional exhaustion is what triggers stress incontinence.
For a hypertonic pelvic floor, forcing more gripping or tightening exercises is like telling someone with a severely cramped shoulder to lift weights. It increases tissue irritation, cuts off healthy circulation, and triggers localized pelvic pain. The primary goal of a trauma-informed practitioner is to first teach these guarded muscles how to fully drop, relax, and lengthen before ever attempting to strengthen them.
3. Trauma-Informed Care: Prioritizing Comfort and Agency
Pelvic floor assessment involves highly personal areas of the body that may hold physical or emotional tension from a difficult labor, birth interventions, or past medical trauma. Because of this, clinical pelvic health must always be guided by strict trauma-informed protocols.
A trauma-informed approach means you are always in complete control of your treatment. Your practitioner should walk through every step of an assessment beforehand, providing a safe, predictable space where your boundaries are fully respected.
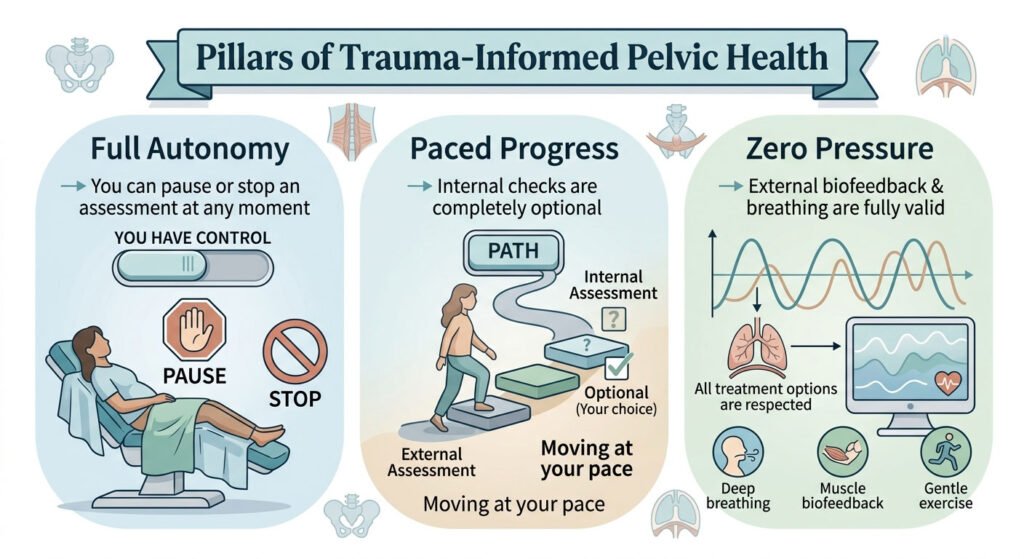
An internal pelvic exam can provide valuable data about muscle tone and strength, but it is never a requirement for successful rehabilitation. A skilled therapist can effectively evaluate and re-educate your pressure system using external observations, physical palpation of the hip stabilizers, and coordinated breathing assessments while keeping you fully clothed and comfortable.
4. Phased Structural Muscle Re-Education Protocol
Restoring your deep core system requires a progressive, mindful rehabilitation timeline that respects tissue healing and nerve reconnection.
1.Phase 1: Down-Training and Diaphragmatic Breath:Calming the System.
Clinical Goal: Lowering defensive muscle guarding and restoring a natural pressure cycle.
Patients learn to perform dedicated diaphragmatic breathing (360-degree breathing). As you breathe in, you consciously visualize your ribs expanding sideways and your pelvic floor fully opening and dropping down. This resets hypertonic muscles and decreases localized tissue irritation.
2.Phase 2: Co-Contraction Coordination:Reconnecting the Core.
Clinical Goal: Teaching the pelvic floor and deep abdominals to fire together naturally.
Once the pelvic floor can relax completely, patients introduce gentle, coordinated core activations. On a slow exhale, you perform a gentle lift of the pelvic floor while drawing the lower belly inward. This trains the base and the front wall to protect your spine automatically during movement.
3.Phase 3: Progressive Dynamic Loading:Functional Integration.
Clinical Goal: Maintaining perfect internal pressure management during everyday activities.
The final phase moves exercises off the therapy table and into real life. Patients practice managing their core pressure during functional movements like squatting, lifting a baby car seat, or climbing stairs, ensuring the body automatically manages internal pressure without leaking or straining.
Clinical Comparison: Integrated Pelvic Care vs. Isolated Care
To help patients build a well-rounded recovery plan, this reference matrix outlines how comprehensive, multi-disciplinary care compares to isolated pelvic exercise:
| Treatment Parameter | Integrated Multi-Disciplinary Care | Isolated Kegel Approach |
|---|---|---|
| Primary Clinical Target | The entire core cylinder, diaphragm, and hips | The isolated puboccocygeus muscle group |
| Hypertonicity Protocol | Lengthens and relaxes high-tone tissue first | Continues to compress already exhausted tissue |
| Assessment Scope | Evaluates posture, pelvic alignment, and breathing | Measures simple, local squeeze power |
| Manual Support Options | Advanced myofascial release of hips and lower back | No complementary soft-tissue work |
| Long-Term Outcome | Restores long-term pressure control and mobility | Can worsen chronic pelvic pain and tension |
The Path to Lasting Physical Restoration
Recovering from childbirth requires looking at the body as an interconnected system. The pelvic floor cannot work efficiently if the surrounding hip bones are rotated, and a tilted pelvis cannot stabilize if the deep abdominal walls are overstretched.
Within the RMT Clinic Network, we navigate post-partum healing using a supportive, collaborative care model. While a Pelvic Floor Physiotherapist works to restore internal coordination and balance your core cylinder, a Registered Massage Therapist (RMT) can simultaneously utilize gentle myofascial release and lymphatic drainage to relieve the deep gluteal tension, lower back stiffness, and fluid retention that naturally accumulate during the post-partum period.
Every stage of your healing journey is documented using secure digital health charting (SOAP notes), keeping your care team perfectly unified. By blending specialized pressure-system re-education, trauma-informed pelvic health, and expert manual therapy, our team addresses both your structural foundation and your overall comfort—giving you a safe, empowering path to reclaim your core strength and live completely pain-free.

Author: Henry Tse
Henry Tse, Founder and CEO of the RMT Clinic Network Organization—an integrated platform created to connect patients with trusted para-medical providers while helping practitioners build stronger, more profitable clinics using practical, real-world business systems. After launching, operating, and selling multiple wellness businesses, I repeatedly saw the same two challenges: patients struggled to find the right care close to them, while practitioners struggled to attract consistent bookings and build predictable, compliant, and sustainable businesses. I created the RMT Clinic ecosystem to solve both problems. Through our Canada-wide “near me” directory, specialized brand marketing solutions, and step-by-step training academy, we help patients discover qualified providers while giving Registered Massage Therapists and clinic owners the systems, tools, and strategies needed to turn their professional skills into scalable businesses. Core Values Innovation • Empowerment • Community Professional Background * Vice President and General Manager, Canadian Small Business Institute: 15 years as a senior business consultant and trainer. * Direct Marketing and Advertising, 1997–Present: Strategy, brand positioning, lead generation, and business development. * Wellness Clinic Owner and Operator, 2005–Present: Launched and operated nine clinics, with three active RMT clinics currently under management. > If you are an RMT or clinic owner looking for more bookings,...